Qualified Abatement Technology
The Logic Layer for
Inpatient Stewardship
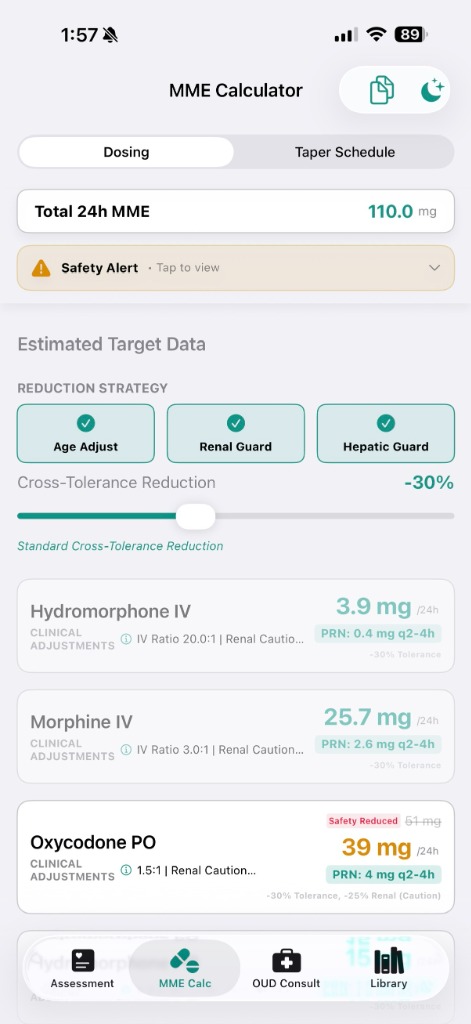
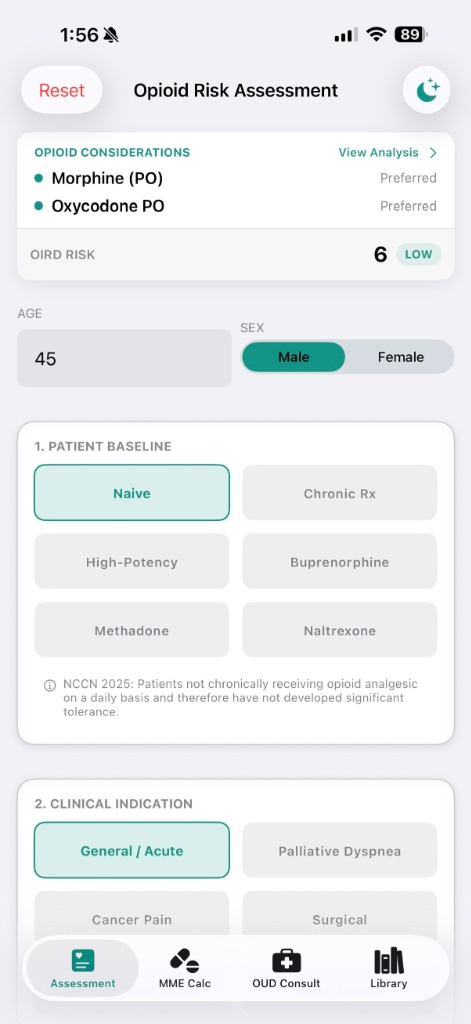
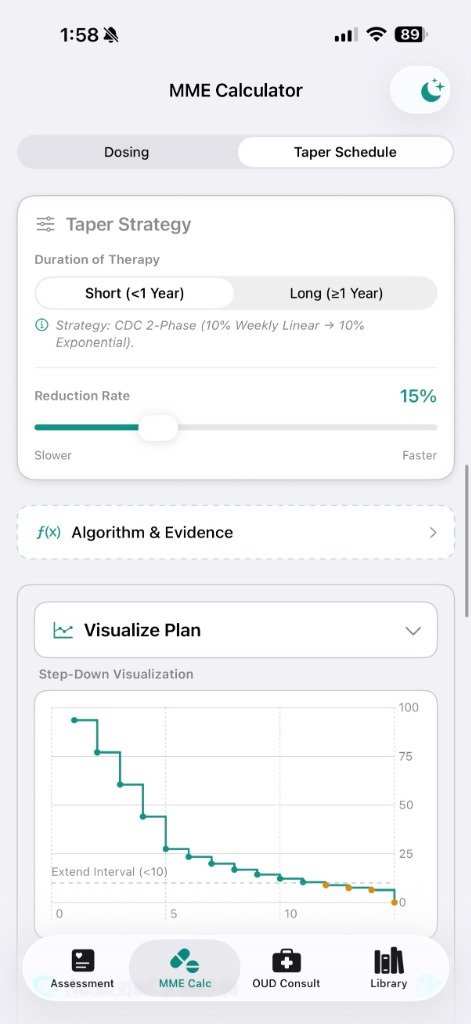
Precision Analgesia resolves the tension between pain management and safety. Replaces manual calculation with EMR-integrated forcing functions to mitigate liability and cost.
For Health Systems
View Integration Guide
For Clinicians
Demo the iOS Beta
Validated against CDC 2022 Clinical Practice Guidelines
Physician-Founded · Addiction Medicine Fellowship, 2026